
One
positive from the air of detachment that pervaded the ward was that no one
seemed to care one way or the other about my ongoing interest in complementary
therapies for Carolie. Both therapists
who treated her in the ICU continued their work in the ward. She responded well to acupuncture and ongoing
vibration healing.

Cognitive signals were strengthening, and encouraging physical responses were apparent, coming as they did from such a low baseline. One of the senior nurse managers visited from the ICU. Her ongoing interest in our welfare was instructive. No neurosurgeon or any other medical interlocutor showed the slightest interest in us once we left their purview, but the ICU nursing corps kept touch and we continued to feel their compassion.
Professional disengagement is one thing - to retain objectivity and
operational clarity - but when it translates to a complete lack of interest in
patient outcomes, it is worrying. I wondered whether patients are viewed as something akin to
inanimate objects on a production line; to be serviced, processed and
dispatched. I continue to ponder this issue.


A
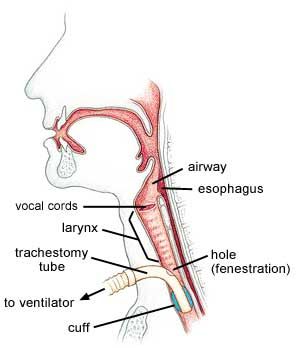
new treatment regime was upon us. Speech
pathologists were at the centre of this next stage in the recovery
process. The challenge was to remove the
tracheostomy at the earliest opportunity without compromising her breathing and
swallowing functions. What had been a
lifesaver was now an impediment to further recovery. Periods for deflation of
the internal sealing cuff increased over several days to encourage Carolie to
breathe for herself – a process monitored closely to clear airways and check
vital signs.
She made good
progress. The way was clear to return to
Canberra with the tracheostomy still in
situ.
I
was both relieved and a little anxious.
I wanted her off this ward as soon as possible. There was something in the general tone of
the place that troubled me. I had become
used to the esprit de corps of the
nursing cohort in the ICU. Their
attention to detail and focussed energies was an ongoing source of
comfort. Ironically, having Carolie at
less risk had not approximated to less worry.
If anything, I was more anxious for her in this ward, surrounded by
discordant noise and static. She
remained extremely vulnerable to infection, was immobile and her cognitive
status was uncertain. Despite the
inherent risks, I had no hesitation in agreeing to a transfer at
the first opportunity. I would not miss this corner of the labyrinth.
An
overhead lifting hoist with harness was a new component in the daily treatment
regime. The contraption operated from
fixed rail runners and enabled nurses to move patients into chairs for
ablutions and other procedures.

The
speech pathologists preferred her sitting up for the airway cuff deflation,
which revealed a serious negative consequence of the aneurysm. Carolie had discernible physical
disability. Her head fell away to the
left and her physical deportment indicated palsy had weakened severely her left
side. This made finding a comfortable
and safe position for cuff deflation more challenging.
Transfers
to chair were simpler because of the harness, but she required close
supervision because of a tendency to collapse to the left. When this occurred, pressure pushed the
tracheostomy tube to an awkward angle, potentially restricting airway
clearance. Her gurgling sounds were
alarming and I frequently called for a nurse to clear the tubes.
It was harrowing at times because the duty
nurse would be busy attending to other patients.
Anxiety would rise until I would have to go looking for someone. Doubtless I need not have been so fearful,
but not having a sense of the relative risks associated with fluid in the
airway left me on edge most of the time.
Muscle wasting further compromised maintenance of her chair posture,
which triggered fits of gurgling that sounded like she was drowning in her own
fluids. The portents for a long and
difficult physical and cognitive rehabilitation were obvious.
To be continued...
No comments:
Post a Comment